
One of the key pieces of information we need when choosing contraception is accurate data on effectiveness. What is the likelihood that your birth control will stop you getting pregnant? We are presented with pretty charts by family planning counsellors, doctors, midwives; sometimes we are told a little more about "real world" and "perfect use" efficacy; if we're lucky, our healthcare workers will do a more individual assessment, giving clear information on how medications, herbal medicines, weight, and other factors might affect contraceptive efficacy.
But how much do we really know about contraceptive failure rates? What do our doctors and nurse practitioners and midwives know? What sources of information are they drawing on? How accurate are those sources? I've typically thought that the sources offered in medical schools and textbooks and review journals and Family Planning leaflets were pretty good; the fact that they took into account real-world differences in use and misuse lent further credibility. Recent information has disabused me of that notion.
The National Prescribing Service (NPS) is a government-funded service in Australia intended to provide practitioners and consumers with independent, evidence-based, accurate education on the Quality Use of Medicines (QUM). It is a service with a lot of reach, and is considered by many doctors to be a rigorous and highly trusted source of medical education. They put out regular bulletins to doctors with information on both new and old drugs.
They have some "information" on contraception that didn't ring true to me. The chart is large, so I've picked out the relevant parts - you can click through for a PDF of the full chart.

See that? Combined oral contraception (COCP, or what most people call the standard "Pill") is cited has having a typical-use failure rate of 8% in the first year; a perfect-use failure rate of 0.3%. Progesterone-only oral contraception (POP, the "mini pill") is cited as having a typical-use failure rate of 8 in the first year and a perfect-use failure rate of 0.3. The vaginal ring with combined hormones is cited as having a typical-use failure rate of 8 in the first year and a perfect-use failure rate of 0.3.
Do you smell a rat too?
[Click through for details on actual rat, size of rat, smelliness of rat, and where the rat came from!]
So I chased and I googled and I tracked, and I think they've just grabbed some contraceptive efficacy data from the World Health Organisation (WHO) website and slapped it in.
See if you can spot the problem with this.
I've excerpted just the barrier and certain female hormonal methods to highlight the problem.

The chart gives identical - not just similar, but identical - figures for failure and discontinuation rates of the combined pill and minipill, the contraceptive patch, and the contraceptive ring, both in typical use and perfect use situations. Typical use failure rate of 8%, perfect use failure rate of 0.3%, discontinuation rate of 68%.
This has to set any half-tuned bullshit-meter a-ringing. There is no study that separates those types of hormonal contraception out, looks at them independently, and comes up with identical rates across the board. They have taken aggregated data for hormonal contraception, then split it for this table.
(The data for nulliparous women using sponges and caps is also identical, and the diaphragm data is close. This also smells.)
The table in the National Prescribing Service educational material for doctors is even worse - they've grabbed the data from this WHO table or its source, then further split out the combined oral contraceptive pill and minipill, attributing them identical failure rates also. Doctors are reading this and "learning" that the minipill (progesterone only pill) is exactly as effective as the combined oral contraceptive pill, then making prescribing decisions on that basis.
You can't grab aggregate data and assume that it applies equally to every subset. That would be like saying that each and every adult human has slightly less than one breast.
I source-chased a little further. With help (thankyou!) I have a Trussell review paper with this chart in it. I have cut it to the relevant parts; click through to see the full chart.
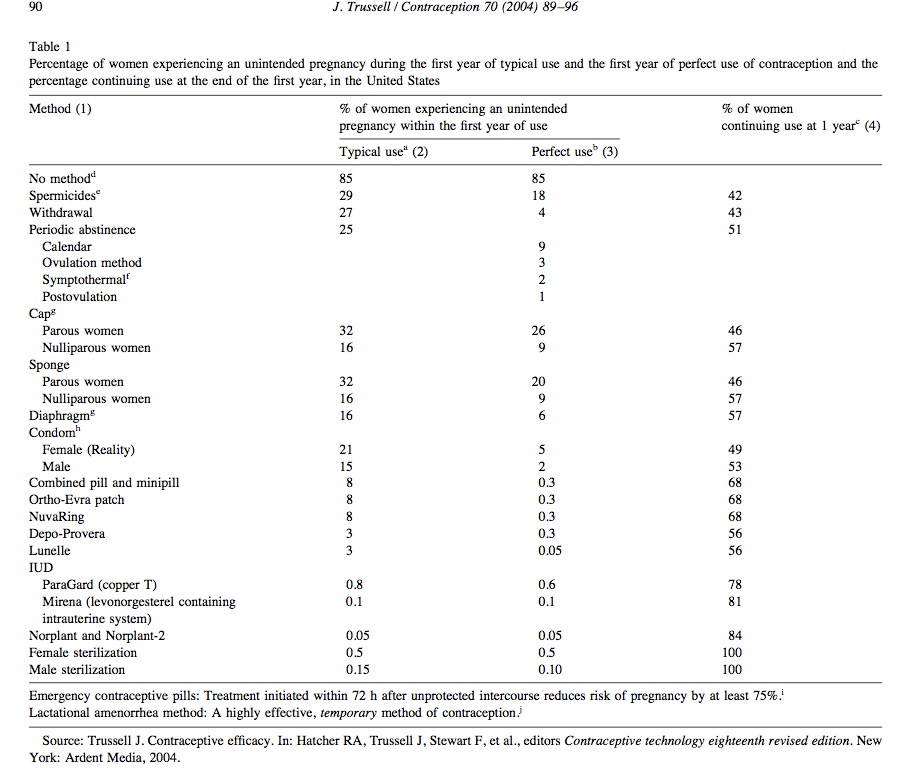
James Trussell, "Contraceptive failure in the United States", Contraception, 2004, 70(2):89-96.
Here are the notes from that source.
"For spermicides, withdrawal, periodic abstinence, the diaphragm, the male condom, the pill and Depo-Provera, these estimates were derived from the experience of women in the 1995 NSFG, corrected for underreporting of abortion, so that the information pertains to nationally representative samples of users [3]. ...Suspicion confirmed. The NPS comparison-chart information on contraceptive efficacy is not evidence-based; it's based on a series of assumptions and estimates and aggregations, and an error of baseless disaggregation that I can't call anything but egregious.
"The NSFG does not ask for brand of pill; thus, combined and progestin-only pills cannot be distinguished. However, because use of the combined pill is far more common than use of the progestin-only pill, the results from the NSFG overwhelmingly reflect typical use of combined pills. The efficacy of progestin-only pills may be lower than that for combined pills because progestin-only pills are probably less forgiving of nonadherence to the dosing schedule. [...]
"The estimates for the Ortho-Evra patch and NuvaRing were set equal to those for the pill. It is possible that the patch and ring will prove to have better efficacy than the pill during typical use, because of better adherence with the dosing schedule. However, such superior efficacy has not been demonstrated in randomized trials. [...] There are no published studies in which women were randomly assigned to the NuvaRing and the pill. Clinical trials of Lunelle cannot yield an estimate of efficacy during typical use, because the design of those trials calls for discontinuing those who return late for their injections [7,8]; the estimate is therefore assumed to be the same as that for Depo-Provera."
Your health dollars at work. Your body at risk.
[Cross-posted.]
~~~
If you're not an Australian local, where are you getting your information on contraceptive efficacy? What does it say? Where does it come from - both immediately, and originally?



Shakesville is run as a safe space. First-time commenters: Please read Shakesville's Commenting Policy and Feminism 101 Section before commenting. We also do lots of in-thread moderation, so we ask that everyone read the entirety of any thread before commenting, to ensure compliance with any in-thread moderation. Thank you.
blog comments powered by Disqus